The Unburdening | Issue 003
The 167-Hour Problem: What Happens Between Sessions
EMILE-E.tech | June 2026 | Audience: Independent Therapists & Small Practices
The Practice Perspective

There are 168 hours in a week.
Your client spends one of them with you.
The other 167 are where their life actually happens — the Tuesday night panic, the difficult conversation they finally had, the small win nobody else noticed. By the time they're back on your couch, half of it has faded, been reframed, or been buried under whatever happened Thursday.
We've talked before about presence in the room. This issue is about what happens outside it — and why the gap between sessions is quietly becoming the defining problem of independent practice in 2026.
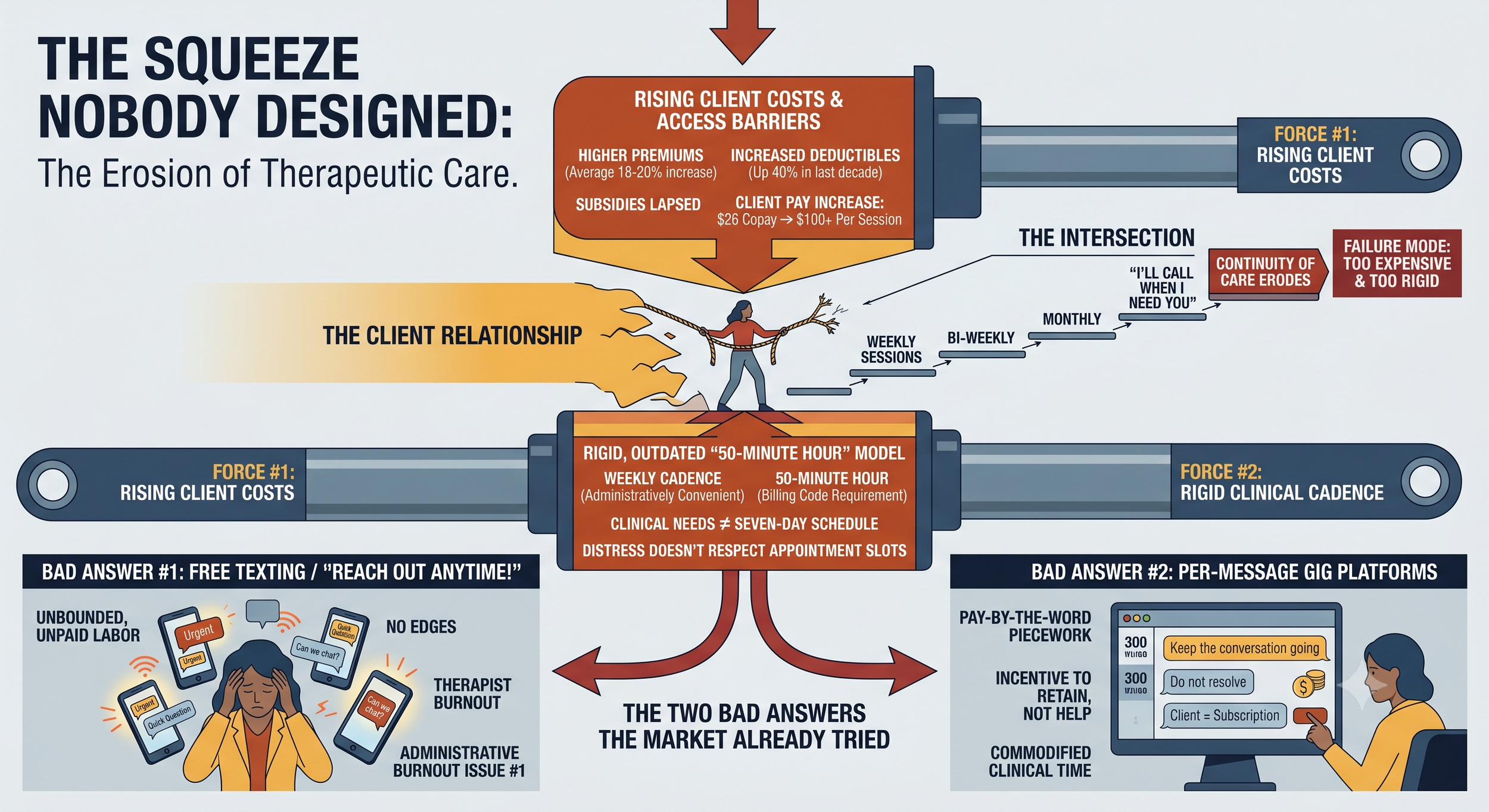
The Squeeze Nobody Designed
Two forces are colliding, and your clients are standing at the intersection.
First, sessions are getting more expensive for the people who need them. Insurers filed for average premium increases of 18–20% heading into 2026, and enhanced federal premium subsidies lapsed at the end of 2025. Deductibles for single coverage have climbed more than 40% over the past decade. The practical result: clients who used to pay a $26 copay are now staring at $100 or more per session — in some cases, more than your sliding-scale rate. One in five Americans now report delaying or avoiding therapy because of insurance complications alone.
Second, weekly cadence was never clinically sacred — it was administratively convenient. Mental health needs do not arrive on a seven-day schedule. The 50-minute hour exists because calendars and billing codes exist. Nobody ever ran the study proving that distress respects appointment slots.
When cost pressure meets a rigid cadence, the failure mode is predictable: clients stretch weekly sessions to bi-weekly, then monthly, then "I'll call when I need you." Continuity of care erodes not because the therapeutic relationship failed — but because the container for it was too rigid and too expensive.
The Two Bad Answers the Market Already Tried
The industry has noticed this gap. Its answers so far should make you nervous.
Bad answer #1: Free texting. "Just reach out anytime!" sounds compassionate and burns therapists alive. Unbounded between-session contact is unpaid labor with no edges — the fastest route from generous clinician to resentful one. We wrote Issue #1 about administrative burnout. Emotional labor without boundaries is the same fire with different fuel.
Bad answer #2: The per-message gig platforms. Venture-scale text therapy apps pay clinicians by the word or by the reply, which creates exactly the incentive you'd expect: keep the conversation going, never resolve anything. The client becomes a subscription to be retained, not a person to be helped. Therapists on these platforms describe it as piecework. Because it is.
Both models fail the same way: they treat between-session contact as either free or infinite. It is neither. It is clinical time — and clinical time deserves structure, boundaries, and fair compensation.
What Good Looks Like: The Continuity Test
At emile-e.tech, we run every idea through The Presence Test (Issue #1). For between-session care, we've added a second filter we call The Continuity Test:
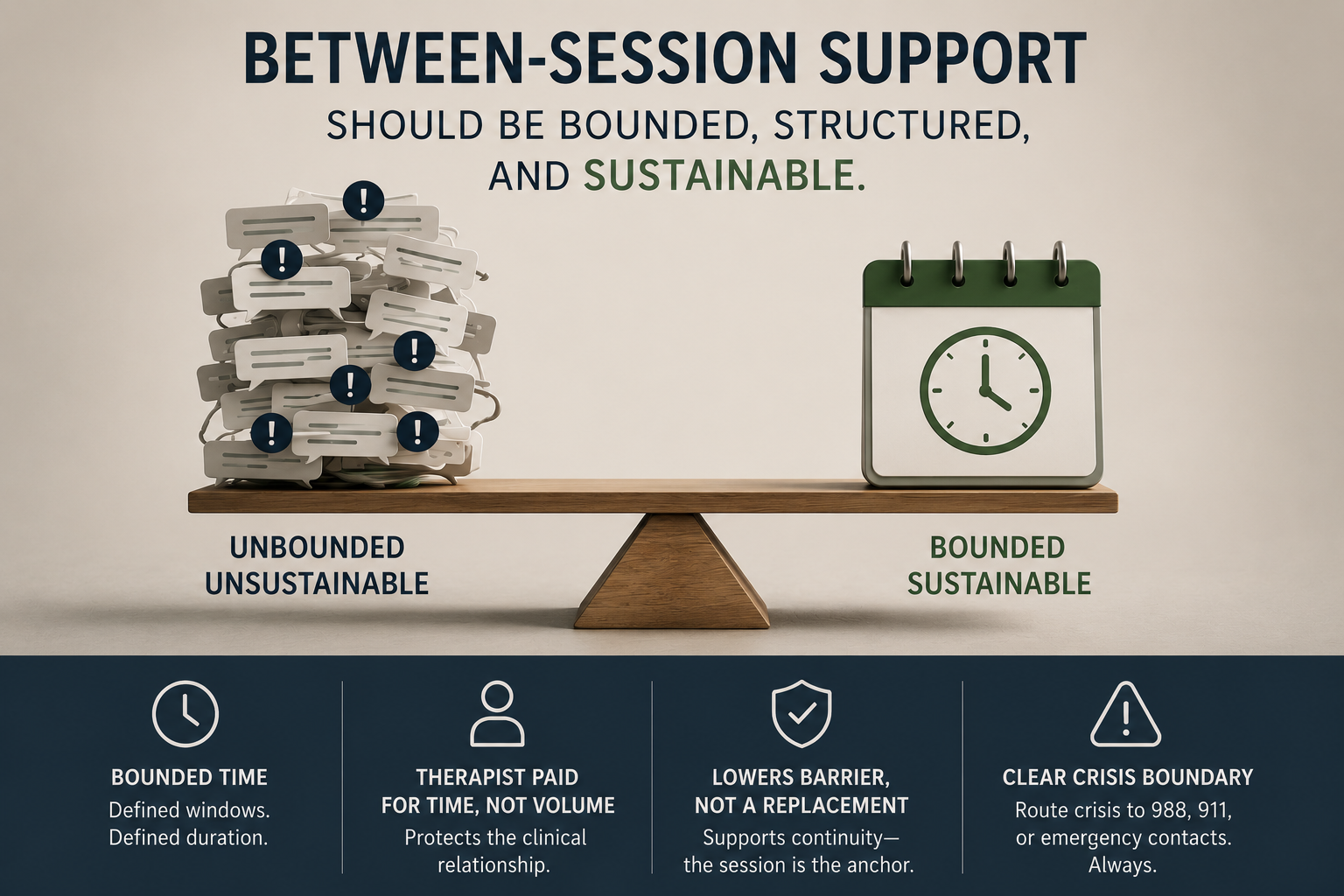
Is the contact bounded? Defined windows, defined duration, a clear beginning and end. A boundary is not a barrier to care — it is what makes care sustainable.
Is the therapist paid for the time, not the volume? Compensation tied to time protects the clinical relationship. Compensation tied to message count corrupts it.
Does it lower the barrier without replacing the anchor? The session remains the foundation. Between-session contact is the connective tissue — a micro-dose of continuity midweek, not a substitute for the room.
Is the crisis line bright and unmistakable? Asynchronous support is not crisis care, and any system that blurs that line is dangerous. Crisis language should route to crisis resources — 988, 911, an emergency contact — immediately and automatically. Always.
If a tool, policy, or platform fails any of these four, it will eventually fail the client, the therapist, or both.
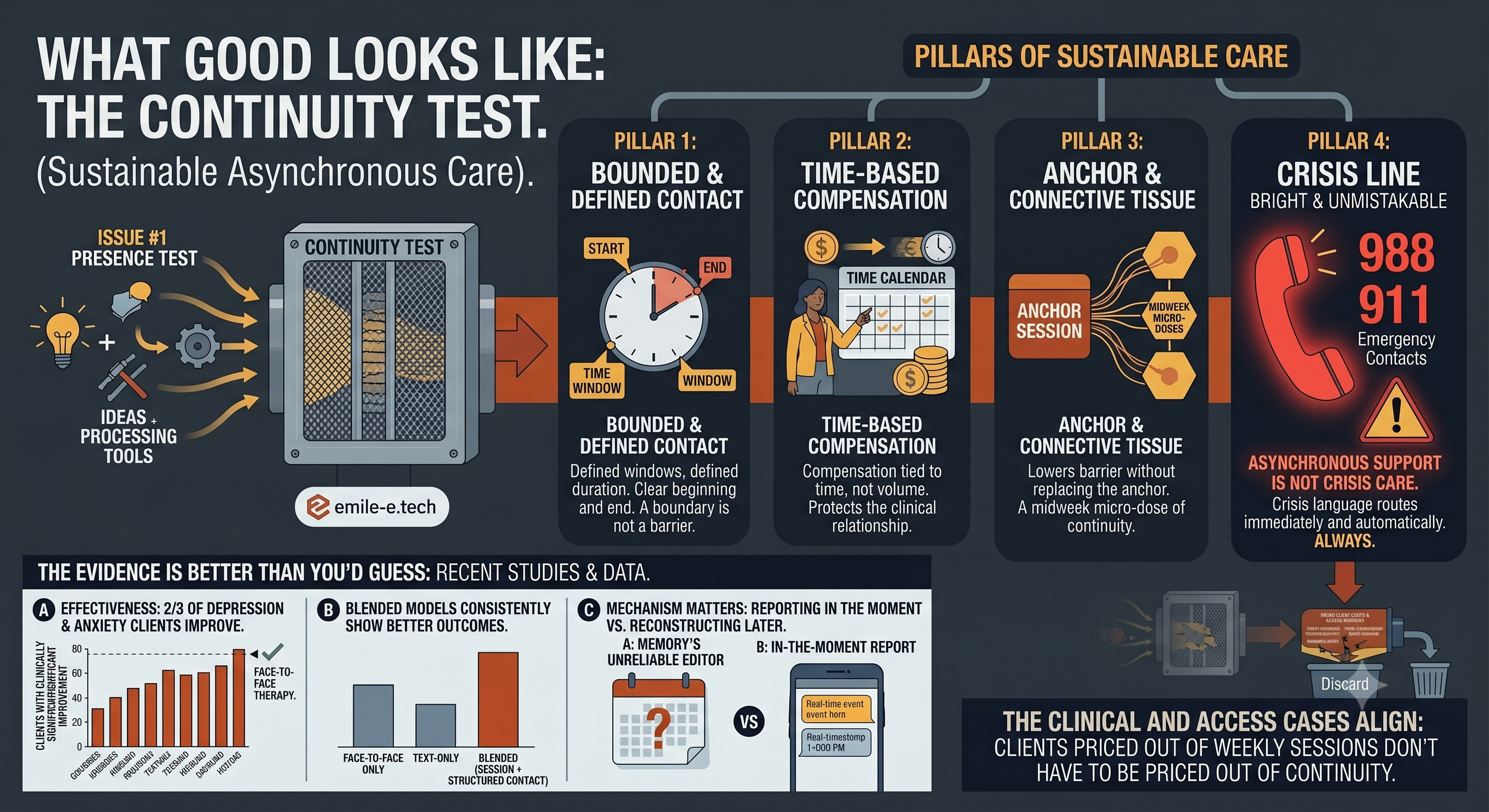
The Evidence Is Better Than You'd Guess
Skepticism about text-based support is healthy. But the research is increasingly hard to dismiss:
In large cohort studies, roughly two-thirds of clients treated for depression and anxiety through structured asynchronous messaging reported clinically significant improvement — rates comparable to face-to-face therapy
Blended models — regular sessions plus structured between-session contact — consistently show better outcomes than either modality alone
The mechanism matters: clients can report experiences in the moment they happen, rather than reconstructing them days later through memory's unreliable editor
The clinical case and the access case point the same direction. A client priced out of weekly sessions doesn't have to be priced out of continuity.
What This Means for Your Practice in 2026
You don't need to wait for software to act on this. Three moves worth making now:
Name your between-session policy. If you don't have one, you have one anyway — it's just undefined, unpaid, and negotiated client-by-client through guilt. Write it down. Defined windows, defined response expectations, defined cost.
Price continuity, don't give it away. A bounded 15-minute midweek exchange is clinical time. Clients losing insurance coverage may keep a lower-cost continuity tier when they can no longer afford weekly sessions. That retains the relationship — and the revenue — that a rigid weekly-or-nothing model loses.
Put the crisis boundary in writing before anything else. Disclaimer at intake, escalation protocol on paper, and clarity for the client about what asynchronous contact is not. This protects them and you.
The practices that thrive through this squeeze will not be the ones that hold the weekly line while clients quietly disappear. They will be the ones that built a flexible, bounded, fairly-priced container around the therapeutic relationship — so the relationship survives the economics.
Where We Go From Here
The Unburdening is a bi-weekly letter on the intersection of clinical practice, technology, and the business of mental health. We write for independent therapists and small practices who are tired of being treated like a billing code — and who believe there is a better way.
We're actively building tools around exactly this problem — bounded, time-tracked, boundary-respecting between-session care. If you want early access and a real voice in how it works, join The Inner Circle, our beta program for therapists who want to shape the platform rather than inherit one.
Until next time — the work matters. And it doesn't stop when the session does.
— The emile-e.tech
References: KFF / ACA Marketplace 2026 premium filings · Grow Therapy Mental Health Benefits Confidence Report (2025) · JMIR / PMC cohort studies on asynchronous messaging psychotherapy · ScienceDirect, CPT-Text for PTSD hybrid effectiveness trial · APA Services policy updates (2026