The Unburdening | Issue 003
The 167-Hour Problem: What Happens Between Sessions
EMILE-E.tech | June 2026 | Audience: Independent Therapists & Small Practices
The Practice Perspective

There are 168 hours in a week.
Your client spends one of them with you.
The other 167 are where their life actually happens — the Tuesday night panic, the difficult conversation they finally had, the small win nobody else noticed. By the time they're back on your couch, half of it has faded, been reframed, or been buried under whatever happened Thursday.
We've talked before about presence in the room. This issue is about what happens outside it — and why the gap between sessions is quietly becoming the defining problem of independent practice in 2026.
The Squeeze Nobody Designed
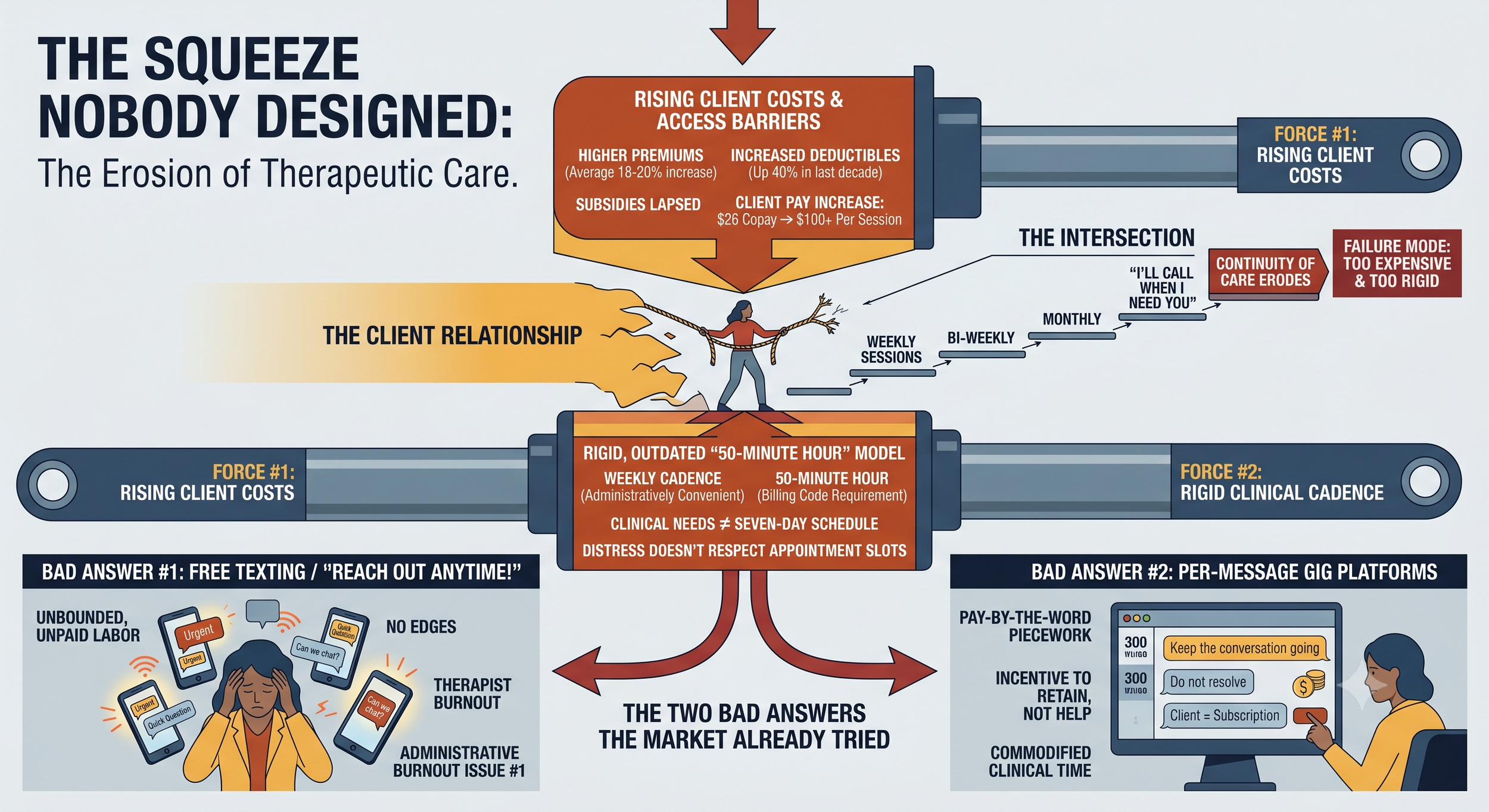
Two forces are colliding, and your clients are standing at the intersection.
First, sessions are getting more expensive for the people who need them. Insurers filed for average premium increases of 18–20% heading into 2026, and enhanced federal premium subsidies lapsed at the end of 2025. Deductibles for single coverage have climbed more than 40% over the past decade. The practical result: clients who used to pay a $26 copay are now staring at $100 or more per session — in some cases, more than your sliding-scale rate. One in five Americans now report delaying or avoiding therapy because of insurance complications alone.
Second, weekly cadence was never clinically sacred — it was administratively convenient. Mental health needs do not arrive on a seven-day schedule. The 50-minute hour exists because calendars and billing codes exist. Nobody ever ran the study proving that distress respects appointment slots.
When cost pressure meets a rigid cadence, the failure mode is predictable: clients stretch weekly sessions to bi-weekly, then monthly, then "I'll call when I need you." Continuity of care erodes not because the therapeutic relationship failed — but because the container for it was too rigid and too expensive.
The Two Bad Answers the Market Already Tried
The industry has noticed this gap. Its answers so far should make you nervous.
Bad answer #1: Free texting. "Just reach out anytime!" sounds compassionate and burns therapists alive. Unbounded between-session contact is unpaid labor with no edges — the fastest route from generous clinician to resentful one. We wrote Issue #1 about administrative burnout. Emotional labor without boundaries is the same fire with different fuel.
Bad answer #2: The per-message gig platforms. Venture-scale text therapy apps pay clinicians by the word or by the reply, which creates exactly the incentive you'd expect: keep the conversation going, never resolve anything. The client becomes a subscription to be retained, not a person to be helped. Therapists on these platforms describe it as piecework. Because it is.
Both models fail the same way: they treat between-session contact as either free or infinite. It is neither. It is clinical time — and clinical time deserves structure, boundaries, and fair compensation.
What Good Looks Like: The Continuity Test
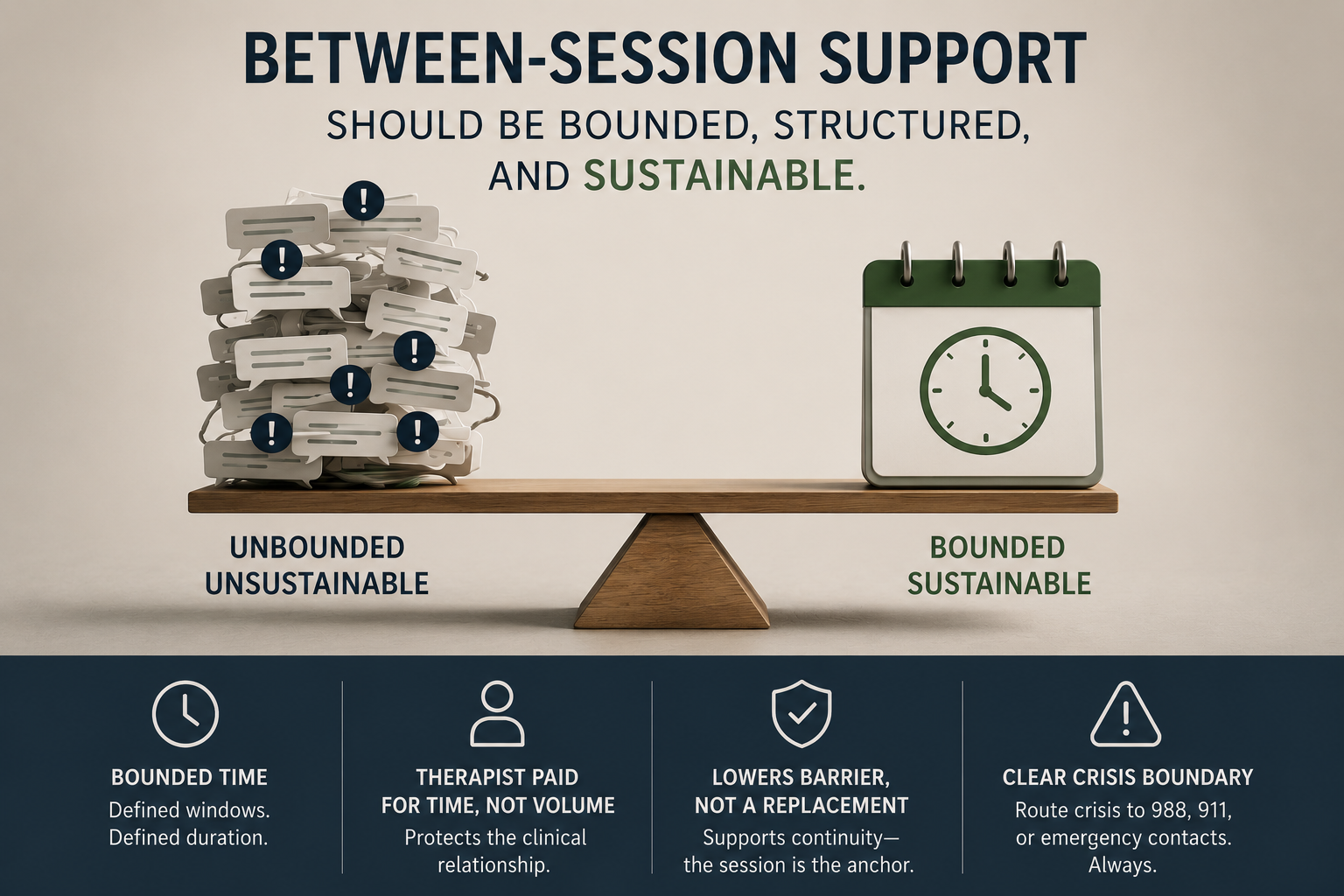
At emile-e.tech, we run every idea through The Presence Test (Issue #1). For between-session care, we've added a second filter we call The Continuity Test:
Is the contact bounded? Defined windows, defined duration, a clear beginning and end. A boundary is not a barrier to care — it is what makes care sustainable.
Is the therapist paid for the time, not the volume? Compensation tied to time protects the clinical relationship. Compensation tied to message count corrupts it.
Does it lower the barrier without replacing the anchor? The session remains the foundation. Between-session contact is the connective tissue — a micro-dose of continuity midweek, not a substitute for the room.
Is the crisis line bright and unmistakable? Asynchronous support is not crisis care, and any system that blurs that line is dangerous. Crisis language should route to crisis resources — 988, 911, an emergency contact — immediately and automatically. Always.
If a tool, policy, or platform fails any of these four, it will eventually fail the client, the therapist, or both.
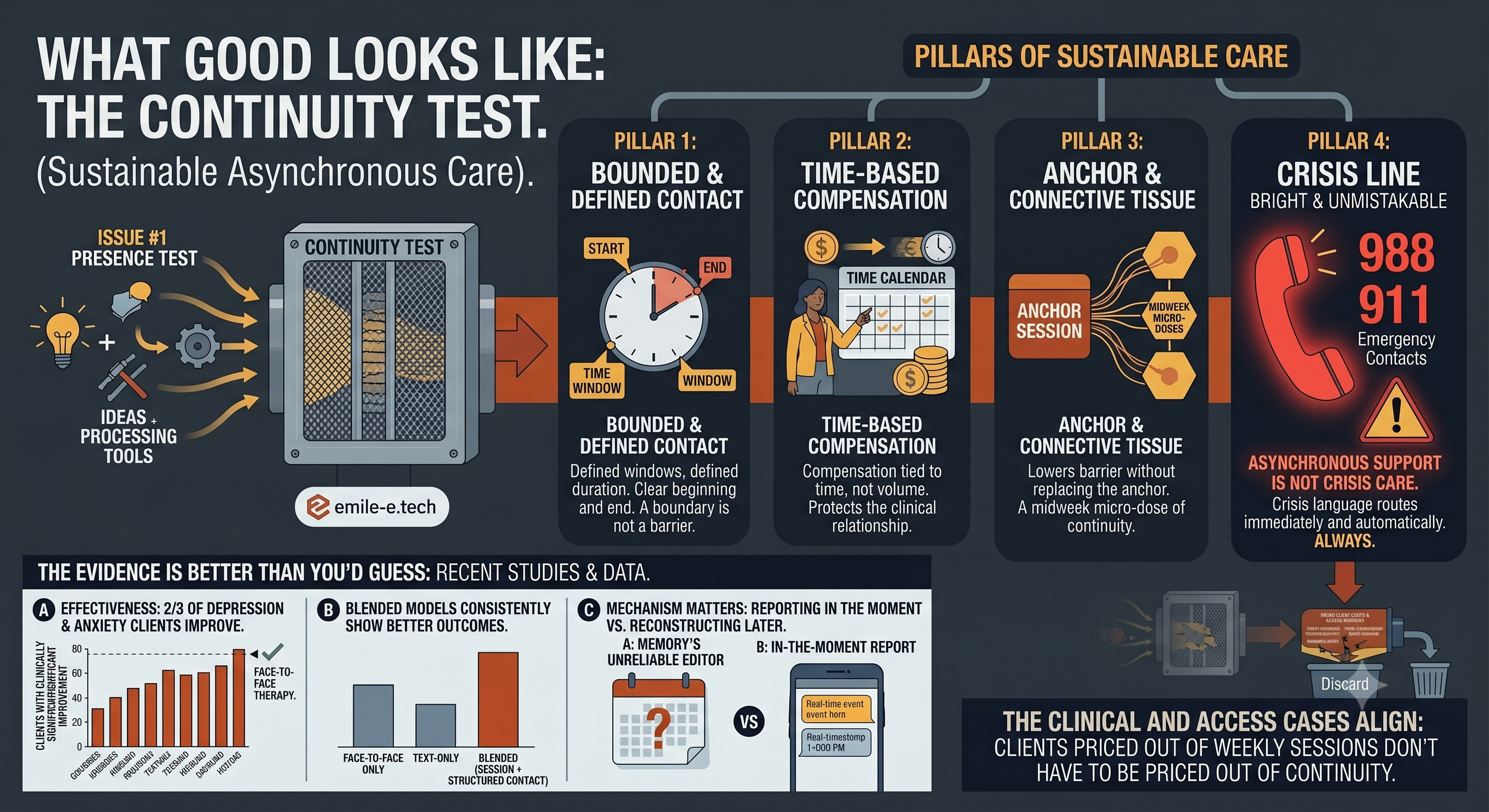
The Evidence Is Better Than You'd Guess
Skepticism about text-based support is healthy. But the research is increasingly hard to dismiss:
In large cohort studies, roughly two-thirds of clients treated for depression and anxiety through structured asynchronous messaging reported clinically significant improvement — rates comparable to face-to-face therapy
Blended models — regular sessions plus structured between-session contact — consistently show better outcomes than either modality alone
The mechanism matters: clients can report experiences in the moment they happen, rather than reconstructing them days later through memory's unreliable editor
The clinical case and the access case point the same direction. A client priced out of weekly sessions doesn't have to be priced out of continuity.
What This Means for Your Practice in 2026
You don't need to wait for software to act on this. Three moves worth making now:
Name your between-session policy. If you don't have one, you have one anyway — it's just undefined, unpaid, and negotiated client-by-client through guilt. Write it down. Defined windows, defined response expectations, defined cost.
Price continuity, don't give it away. A bounded 15-minute midweek exchange is clinical time. Clients losing insurance coverage may keep a lower-cost continuity tier when they can no longer afford weekly sessions. That retains the relationship — and the revenue — that a rigid weekly-or-nothing model loses.
Put the crisis boundary in writing before anything else. Disclaimer at intake, escalation protocol on paper, and clarity for the client about what asynchronous contact is not. This protects them and you.
The practices that thrive through this squeeze will not be the ones that hold the weekly line while clients quietly disappear. They will be the ones that built a flexible, bounded, fairly-priced container around the therapeutic relationship — so the relationship survives the economics.
Where We Go From Here
The Unburdening is a bi-weekly letter on the intersection of clinical practice, technology, and the business of mental health. We write for independent therapists and small practices who are tired of being treated like a billing code — and who believe there is a better way.
We're actively building tools around exactly this problem — bounded, time-tracked, boundary-respecting between-session care. If you want early access and a real voice in how it works, join The Inner Circle, our beta program for therapists who want to shape the platform rather than inherit one.
Until next time — the work matters. And it doesn't stop when the session does.
— The emile-e.tech
References: KFF / ACA Marketplace 2026 premium filings · Grow Therapy Mental Health Benefits Confidence Report (2025) · JMIR / PMC cohort studies on asynchronous messaging psychotherapy · ScienceDirect, CPT-Text for PTSD hybrid effectiveness trial · APA Services policy updates (2026
The Unburdening | Issue 002
Secure AI Is Not a Feature
EMILE-E.tech | 📅 May 2026 | Publication Date: May 8, 2026
Secure AI Is Not a Feature. It Is a Clinical Responsibility.

Secure AI in behavioral health starts with trust, boundaries, and accountability.
AI is moving into behavioral health whether practices are ready or not. Some tools are arriving through official vendor channels. Others are slipping in quietly through browser tabs, copied notes, intake summaries, staff experiments, and “just this once” shortcuts that eventually become workflow.
That matters because behavioral health data is not ordinary data. It carries diagnoses, trauma histories, substance use treatment details, family systems, medications, safety plans, and disclosures people may have never shared anywhere else. If AI is going to touch that environment, “secure” cannot mean a logo on a sales page. It has to mean governance, safeguards, accountability, and clinical context from the beginning.
The Compliance Floor Is Rising
For behavioral health practices, 2026 is not just another year of vague AI anxiety. It is a year when privacy, security, and substance use confidentiality expectations are becoming more concrete.
Updated enforcement around 42 CFR Part 2 began on February 16, 2026, bringing renewed attention to how substance use disorder treatment records are handled, disclosed, segmented, and protected. At the same time, OCR has continued signaling focus on HIPAA risk analysis, risk management plans, and the real operational controls organizations use to protect electronic protected health information.
AI now belongs inside that risk conversation.
A serious AI risk analysis should ask basic but uncomfortable questions:
What AI tools are staff actually using?
Is PHI being entered into systems that are not approved?
Do vendors sign Business Associate Agreements when required?
Are prompts, outputs, and uploaded documents retained or used for model training?
Can the practice audit access and activity?
Are Part 2 records handled differently where required?
Who owns the decision when AI output is wrong?
That is not bureaucracy for its own sake. It is the difference between a helpful tool and an unmanaged disclosure pathway.
“Secure AI” Means More Than Encryption
Encryption matters. So do access controls, secure APIs, and hardened infrastructure. But in behavioral health, security also has to understand clinical boundaries.
A generic AI tool may be technically impressive and still be unsafe for practice use. If it stores prompts indefinitely, trains on submitted content, lacks a BAA, provides no audit trail, or cannot respect consent restrictions, it does not belong anywhere near PHI.
Secure AI for behavioral health should include several layers.
First, API security has to be intentional. Connections between the EHR, AI services, document systems, scheduling tools, and internal applications should use secure authentication, least-privilege access, scoped tokens, and careful permissioning. A tool should not get broad access to the entire clinical record when it only needs a limited data element for a specific workflow.
Second, audit logging should be non-negotiable. Practices need to know who accessed what, when they accessed it, what system action occurred, and whether data moved outside an approved boundary. If an AI tool generates a summary, drafts a message, or processes an intake packet, that activity should not disappear into a black box.
Third, prompt and model data handling must be explicit. Practices should know whether prompts are stored, how long outputs are retained, whether data is used to train models, whether subprocessors are involved, and what happens when information is deleted. “We use AI” is not enough. The details matter.
Fourth, BAAs still matter. If a vendor creates, receives, maintains, or transmits PHI on behalf of a covered entity, the compliance conversation cannot stop at convenience. A signed Business Associate Agreement is not a magic shield, but the absence of one is often a warning sign that the vendor is not prepared for healthcare use.
Part 2 Changes the Design Problem

Consent-aware segmentation is part of safe AI design, not a secondary feature.
HIPAA is already complex. 42 CFR Part 2 adds another layer because it protects substance use disorder treatment records with heightened confidentiality requirements.
This is where many AI workflows can break down if they are designed too casually.
A practice might want AI to summarize a client chart before a session. That sounds useful. But what if part of that chart includes Part 2 protected information? What if the client consented to share general behavioral health information with one provider, but not substance use treatment details with another? What if an AI assistant pulls everything into one combined summary without respecting consent boundaries?
That is why consent-aware data segmentation matters.
A safer system should be able to distinguish categories of data, honor consent rules, restrict what is surfaced to which user, and prevent sensitive records from being blended into outputs that travel too far. This is not only a technical concern. It is a trust concern. Clients should not have to wonder whether a tool buried inside the practice stack is quietly ignoring the boundaries they were promised.
For AI integration, this means the EHR connection cannot be treated as a simple data pipe. It needs context. It needs rules. It needs access logic. It needs to understand that “available in the chart” does not always mean “appropriate for this use.”
The Shadow AI Problem Is Already Here
Most practices do not adopt risky AI because they are reckless. They do it because people are tired.
A clinician has six notes left after dinner. An intake coordinator is buried under forms. A biller is trying to interpret messy documentation. An owner is trying to keep the practice solvent while fielding vendor pitches from every direction. Someone finds a tool that saves time, and the relief is immediate.
That is exactly why practices need a better path than saying either “ban all AI” or “let everyone figure it out.”

The safer path is not banning AI, but making responsible use easier than improvisation.
A practical AI governance plan can start small:
Build an inventory of approved and unapproved AI tools
Define what staff may never enter into public AI systems
Review vendor BAAs, retention terms, model training policies, and audit rights
Add AI risks to the HIPAA security risk analysis
Create a risk management plan with owners and timelines
Train staff on real examples, not abstract fear
Establish a review process before new AI tools touch PHI
The goal is not to scare people away from useful technology. The goal is to make safe use easier than unsafe improvisation.
Mental Health Deserves Better Than Rushed AI
Behavioral health has been asked to tolerate bad software for too long. Clunky portals. Duplicative documentation. Fragmented systems. Tools that technically function but make human work harder.
AI should not become the next version of that problem.
Done well, AI can reduce administrative load, improve operational clarity, help staff find information faster, and make practice systems feel less hostile. Done poorly, it can leak PHI, flatten clinical nuance, undermine consent, and create compliance exposure that practice owners only discover after damage is done.
The difference is not whether a product says “AI.” The difference is whether it was built with healthcare reality in mind.
That means security and compliance are not add-ons. Clinical context is not decoration. Ethical design is not marketing language. For mental health practices, these are the foundation.
At EMILE-E.tech, this is the work we care about: helping behavioral health practices use AI in ways that are safe, reliable, and grounded in the real pressures of clinical operations. We believe mental health deserves technology that protects trust instead of putting it at risk.
Closing Thought
The future of AI in behavioral health will not be defined by the flashiest demo. It will be defined by whether practices can adopt powerful tools without compromising the privacy, consent, and dignity of the people they serve. Secure AI is not about slowing innovation down. It is about making sure innovation is worthy of the room it is entering.
Garry Gilbert Jr.
Founder, EMILE-E.tech
If your practice is thinking about AI but wants to do it carefully, EMILE-E.tech is building for that exact space. Visit EMILE-E.tech to learn more about secure, ethical AI integration for mental health practices.
The Unburdening | Issue 001
The 2026 Shift: From Efficiency to Presence
EMILE-E.tech | 📅 April 2026 | Audience: Independent Therapists & Small Practices
The Cost of “Efficiency” in Therapy
There is a quiet crisis happening in mental health practices across the country.
Therapists who got into this work because they wanted to help people are now spending their evenings and weekends documenting. Filling out fields. Clicking through portals designed for billing departments, not for healers.
The industry called it "efficiency." For five years, the promise was: more sessions, better throughput, scaled practices.
2026 is turning that promise on its head.
The Shift Nobody is Talking About (Yet)
The most sophisticated behavioral health operators in the country are making a quiet pivot. Not toward more technology, toward less of the right technology. They are measuring success differently: not in sessions-per-week, but in quality-of-presence. Not in claims processed, but in whether the therapist walked into the room, mentally and emotionally, ready to receive another human being.
This is the shift we built emile-e.tech around. And the market is starting to catch up.
What Changed?
Three forces converged in late 2025 and early 2026:
Clinician burnout hit a breaking point. The American Psychological Association's 2025 Workforce Survey found that 61% of independent practitioners reported feeling "chronically over-extended." The primary driver? Administrative burden, not caseload.
AI tools flooded the market, and most of them made things worse. Generative AI transcription tools promised to "eliminate documentation." What they delivered was a second layer of work: reviewing, editing, and correcting AI-generated SOAP notes that missed the nuance of a therapeutic moment. Clinicians started calling it "AI-generated busywork."
The "Invisible UI" philosophy started gaining traction. Pioneered by patient-facing health systems that serve fragile populations (pediatric, geriatric, crisis), the principle is simple: technology should ask for less attention, not more. If a client has to navigate a portal to upload a feeling, the portal has already failed.
The Three Questions We Ask Before Every Feature
At emile-e.tech, every product decision runs through a filter we call The Presence Test:
Does this reduce cognitive load at the moment of care? Or does it add a field to fill out, a button to click, a portal to navigate?
Who is this serving; the billing department or the healing relationship? Both matter. But when they conflict, we default to the healing relationship.
Could a patient in crisis use this without external support? If the answer is no, we redesign. Complexity is a barrier.
This is why our AI assistance model is built on the principle of ambient intelligence, not ambient surveillance. The technology is present. It observes, contextualizes, and prepares, but it does not interrupt. The therapist is always the final author. The document is always theirs to shape.
The Numbers Behind the Shift
From the APA Monitor (January 2026):
78% of therapists report that administrative tools are the primary source of their workday dissatisfaction
3.2 hours per day is the average time an independent therapist spends on EHR-related tasks in a solo practice
$18,400 per year is the estimated cost of billing-related administrative overhead for a small solo practice (1-3 clinicians)
The ROI case for "doing less with technology" is stronger than the case for "more efficiency." Reducing administrative friction by even 40% is equivalent to adding one session per day — without adding a single new client.
What This Means for Your Practice in 2026
The independent practices that thrive over the next three years will not be the ones that adopted the most AI tools. They will be the ones that chose the right technology, tools that disappear into the background, that handle the administrative complexity so the clinician can be fully present.
This is the work we are building. Not because we believe technology will fix mental health care. But because we believe the right technology can remove the barriers that prevent healers from doing what they were trained to do.
The Bottom Line
The Unburdening is a bi-weekly letter on the intersection of clinical practice, technology, and the business of mental health. We write for independent therapists and small practices who are tired of being treated like a billing code, and who believe there is a better way.
If this resonated with you, we invite you to join The Inner Circle; our beta program for therapists who want early access to our platform and direct input on how we build it.
Until next time, the work matters. The technology should get out of the way.
— The emile-e.tech
References: APA Monitor (Jan 2026) · Nature Medicine (AI & Therapy, 2025/2026) · Grow Therapy 2026 Report · ASTP/ONC BHIT Pilots (Feb 2026) · SimplePractice Equity Data
Protecting Your Practice: Why Email Security Matters More Than You Think
Running a private practice means wearing many hats. You’re not only a therapist, counselor, or psychologist—you’re also a small business owner managing schedules, billing, insurance, and everything in between. That’s a lot already. The last thing you probably want to think about is cybersecurity.
But here’s the reality: most cyber attacks on small businesses, including mental health practices, start with something as ordinary as email.
Why Emails Are Such a Big Risk
Think about how much important information flows through your inbox every day. Appointment reminders, insurance paperwork, intake forms, medication lists—it’s all there. Hackers know that, and they’ve gotten very good at creating emails that look real but are actually traps. 🪤
For mental health providers, the risks are especially high because the information you handle is so sensitive. If someone gains access, it’s not just data—it’s your clients’ trust and privacy at stake.
What These Emails Usually Look Like
Here are a few common tricks cybercriminals use to sneak into inboxes:
Phishing emails – Messages that might look like they’re from an insurance company, a billing service, or even a colleague, asking you to click a link or enter a password.
Fake attachments – Documents that appear to be referral letters or intake forms but actually contain harmful software once opened.
Imposter messages – An email that seems to come from you or a colleague, asking staff to send sensitive information or make a payment.
They often look “official” and can be hard to spot, especially when you’re busy.
What Could Happen if One Slips Through
Even one successful email attack can cause a ripple effect. It might mean:
Losing access to your email—or worse, your entire computer system—for days.
Needing to notify clients about a data breach (which no one wants to do).
Facing potential HIPAA headaches and even fines.
Dealing with lost income and a whole lot of stress.
And as a provider, the biggest toll might not be financial—it’s the erosion of trust with the people you’re there to help.
Practical Steps You Can Take (No Tech Degree Required)
Here are a few manageable ways to protect your practice:
Pause before clicking. If an email seems “off,” even a little, double-check before opening links or attachments.
Use two-step logins. Multi-factor authentication (MFA) might sound fancy, but really, it just means a second check (like a code texted to your phone) before logging in. It’s one of the easiest ways to keep hackers out.
Update your software. Those little reminders to update your computer or email app aren’t just annoying—they actually patch security holes that hackers love to use.
Keep patient info off regular email. When possible, use a secure messaging system or portal for sharing protected health information.
Have a “what if” plan. Decide ahead of time how you and your staff will react if you think an email account’s been hacked.
You Don’t Have to Figure This Out Alone
Cybersecurity can feel overwhelming, but you don’t have to be an expert to keep your practice safe. Small, consistent steps make a big difference.
At EMILE-E.tech, we work specifically with healthcare providers who want peace of mind without all the jargon. Our job is to set up the tools and training you need, so you can focus on what truly matters—caring for your clients.
Because at the end of the day, email safety isn’t about “tech.” It’s about protecting the trust you’ve built with the people who rely on you. 🤝💪🏻

Garry Gilbert Jr
More about the founder.

Garry Gilbert Jr.
Founder and CEO of EMILE-E
CTO of Meridian Counseling Center.